Predictive Sovereignty: The Rise of the AI-Native Healthcare Cloud
By Vatsal Shah · June 26, 2026 · Business / Healthcare
Table of Contents
- Introduction: The 'Privacy-Performance' Paradox in Medical AI
- The Architecture of Sovereign Patient Data Lakes
- Localized LLMs for Diagnosis: Keeping Intelligence On-Premises
- The Virtual Health Twin: Simulating Complex Treatments at the Edge
- Real-Time Pandemic Surveillance: Decentralized Global Safety Networks
- Comparative Architecture: Legacy EMR vs. AI-Native Healthcare OS
- Futuristic Roadmap: The 2030 'Zero-Waiting-Room' Hospital
- Actionable Close: Monday Morning Steps for MedTech Leaders
Introduction: The 'Privacy-Performance' Paradox in Medical AI
For a decade, the healthcare industry has been trapped in a paralyzing architectural paradox. On one side stands the promise of generative artificial intelligence: predictive diagnostic loops, real-time clinical summarization, and autonomous scheduling engines that can wipe out administrative burnout. On the other side stands the fortress of regulatory compliance: HIPAA, HITECH, GDPR, and the absolute ethical mandate of patient privacy.
Traditional cloud computing architectures cannot solve this. The moment you route identifiable patient records (PHI) across the public internet to a third-party LLM API, you create a sprawling digital attack surface. Yet, restricting clinical systems to isolated, legacy databases leaves hospitals stuck in a pre-AI dark age of manual data entry and disjointed workflows. I’ve seen this fail repeatedly in hospital settings: cloud connections lag in critical moments, WAN outages freeze diagnostic helper tools, and legal departments block the rollout of powerful tools out of fear of data leakage.
In 2026, a new architectural paradigm has emerged to resolve this tension: Predictive Sovereignty.
Predictive Sovereignty is the systematic containment of diagnostic intelligence and patient records within a physical and logical sovereign boundary. It means that the model comes to the data, not the other way around. By combining high-performance localized Small Language Models (SLMs), micro-segmented edge compute hardware, and decentralized data fabrics, forward-thinking medical groups are deploying the first true AI-Native Healthcare Clouds.
This guide lays out the concrete technical blueprints for this transformation. We will dissect how to design edge-first data pipelines, run zero-latency diagnostic models inside hospital walls, simulate clinical treatments via virtual health twins, and execute global threat intelligence using federated, privacy-preserving networks.
The Architecture of Sovereign Patient Data Lakes
The foundation of an AI-native healthcare cloud is the Sovereign Patient Data Lake. Traditional Electronic Health Record (EHR) databases are relational silos, poorly structured for raw vector embeddings or contextual model retrieval. In contrast, a sovereign data lake ingests structured HL7 FHIR (Fast Healthcare Interoperability Resources) feeds, unstructured clinical notes, imaging metadata, and streaming IoT telemetry into a single, localized object store.
Physical and Logical Containment
To maintain predictive sovereignty, the data lake must reside on physical edge nodes inside the hospital's local network. This is not a return to legacy server cupboards; it is the deployment of micro-cloud platforms (such as edge servers backed by local Kubernetes clusters) that operate autonomously from the internet.
[ Local Hospital Network Boundary ]
+-------------------+ +----------------------+ +---------------------+
| Edge Devices | | Sovereign Data Lake | | Local Neural Engine |
| - Vital Sensors | =====> | - Raw Object Store | =====> | - Diagnostic SLMs |
| - Clinical Tablets| (FHIR)| - Encrypted DBs | (Local)| - Vector Databases |
+-------------------+ +----------------------+ +---------------------+
||
|| (Isolated Transit)
\/
+----------------------+
| HIPAA/GDPR Lock Gate |
| - Zero-Trust Guard |
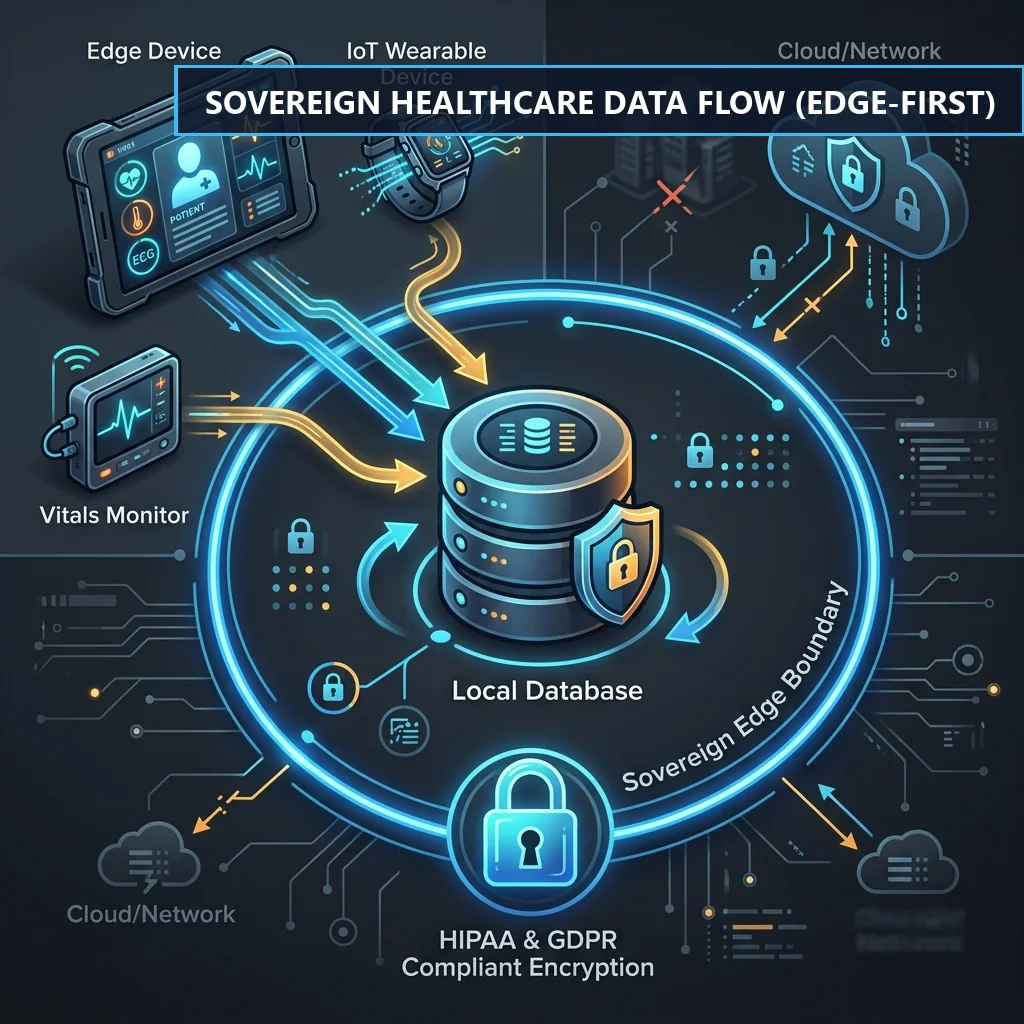
+----------------------+The data flow works on an Edge-First principle:
- All clinical telemetry, notes, and records are written directly to local physical volumes.
- An on-device ETL engine parses FHIR JSON structures and maps them into localized vector stores (such as pgvector or Qdrant running on-site).
- The cryptographic keys governing the databases are managed via local HSM (Hardware Security Module) devices. Cloud providers or external vendors have zero access to the decryption keys.
Cryptographic Micro-segmentation
To prevent lateral movement inside the network during a breach, patient data is segmentally encrypted at the record level. Every patient profile is assigned a unique, cryptographically isolated namespace.
Let us look at a structural policy layout using Cedar or Open Policy Agent (OPA) to enforce localized zero-trust boundaries:
# OPA Policy enforcing Localized Healthcare Data Boundaries
package healthcare.sovereignty
default allow_access = false
# Allow local clinicians to read PHI if within hospital boundary
allow_access {
input.subject.role == "clinician"
input.resource.classification == "PHI"
input.request.location == "on-premises"
input.request.network_status == "secure-local-tunnel"
is_valid_namespace(input.subject.id, input.resource.patient_id)
}
# Block all external cloud access attempts to unanonymized PHI
allow_access = false {
input.request.origin == "cloud-api-gateway"
input.resource.is_anonymized == false
}
is_valid_namespace(clinician_id, patient_id) {
# Check localized active assignments list
assignments := data.active_clinical_assignments[clinician_id]
assignments[_] == patient_id
}By putting strict compliance policies directly into code, we ensure that raw patient data can never exit the physical local environment.
Localized LLMs for Diagnosis: Keeping Intelligence On-Premises
Running clinical models in the cloud is a regulatory risk and a latency liability. A doctor waiting for a real-time prescription check or an emergency room router cannot depend on a model hosted on an external server. The solution is running domain-specific Small Language Models (SLMs) directly on local hardware.
Hardware-Accelerated Local Inference
In 2026, local silicon performance has crossed a critical threshold. High-density edge computers and local workstations equipped with unified memory architectures can easily run quantized 7B to 13B parameter models at speeds exceeding 80 tokens per second.
+--------------------------------------------------------------------------+
| Local Edge Workstation |
| |
| +-----------------------+ +---------------------+ |
| | Unified Memory (RAM) | <===============> | GPU / Neural Engine | |
| | - Quantized SLM Model| High-Bandwidth | - Matrix Math Units | |
| | - Clinical Vector DB | Silicon | - Tensor Execution | |
| +-----------------------+ +---------------------+ |
+--------------------------------------------------------------------------+By leveraging local memory configurations, we bypass the need for external network calls entirely. The diagnostic application queries the model running locally, protecting patient privacy by design while ensuring high-speed processing.
Custom Clinical Fine-Tuning
While generic public models are broad, local clinical models are deep. A local 8B model fine-tuned on custom clinical notes and medical textbooks consistently beats a generic 70B model in identifying specific medical conditions and mapping treatments.
Here is an example python script using a local setup to execute clinical entity extraction and routing, ensuring that all data processing is localized:
import os
import json
from transformers import AutoModelForCausalLM, AutoTokenizer
import torch
class LocalClinicalExtractor:
def __init__(self, model_path: str):
# Load local model and tokenizer using Apple Silicon / local CUDA
self.device = "cuda" if torch.cuda.is_available() else "mps" if torch.backends.mps.is_available() else "cpu"
self.tokenizer = AutoTokenizer.from_pretrained(model_path)
self.model = AutoModelForCausalLM.from_pretrained(
model_path,
torch_dtype=torch.float16 if self.device != "cpu" else torch.float32
).to(self.device)
def extract_phi_context(self, clinical_notes: str) -> dict:
prompt = f"""[INST] You are an on-premises clinical entity extractor.
Extract all clinical entities from the patient notes below. Do not output raw PHI identifier values directly, only key symptoms and disease codes.
Notes:
{clinical_notes}
[/INST]"""
inputs = self.tokenizer(prompt, return_tensors="pt").to(self.device)
with torch.no_grad():
outputs = self.model.generate(
**inputs,
max_new_tokens=256,
temperature=0.1,
do_sample=False
)
response = self.tokenizer.decode(outputs[0][inputs.input_ids.shape[1]:], skip_special_tokens=True)
try:
return json.loads(response)
except json.JSONDecodeError:
# Fallback parsing logic
return {"raw_output": response}
# Instantiation within the local hospital security network
if __name__ == "__main__":
# Pointing to local workspace weights
extractor = LocalClinicalExtractor(model_path="/opt/models/clinical-llama-8b-quant")
sample_notes = "Patient presents with persistent dyspnea and tachycardia. Elevated troponin levels detected."
result = extractor.extract_phi_context(sample_notes)
print(json.dumps(result, indent=2))This local processing pipeline guarantees that the clinical notes are parsed inside the hospital's local compute node.
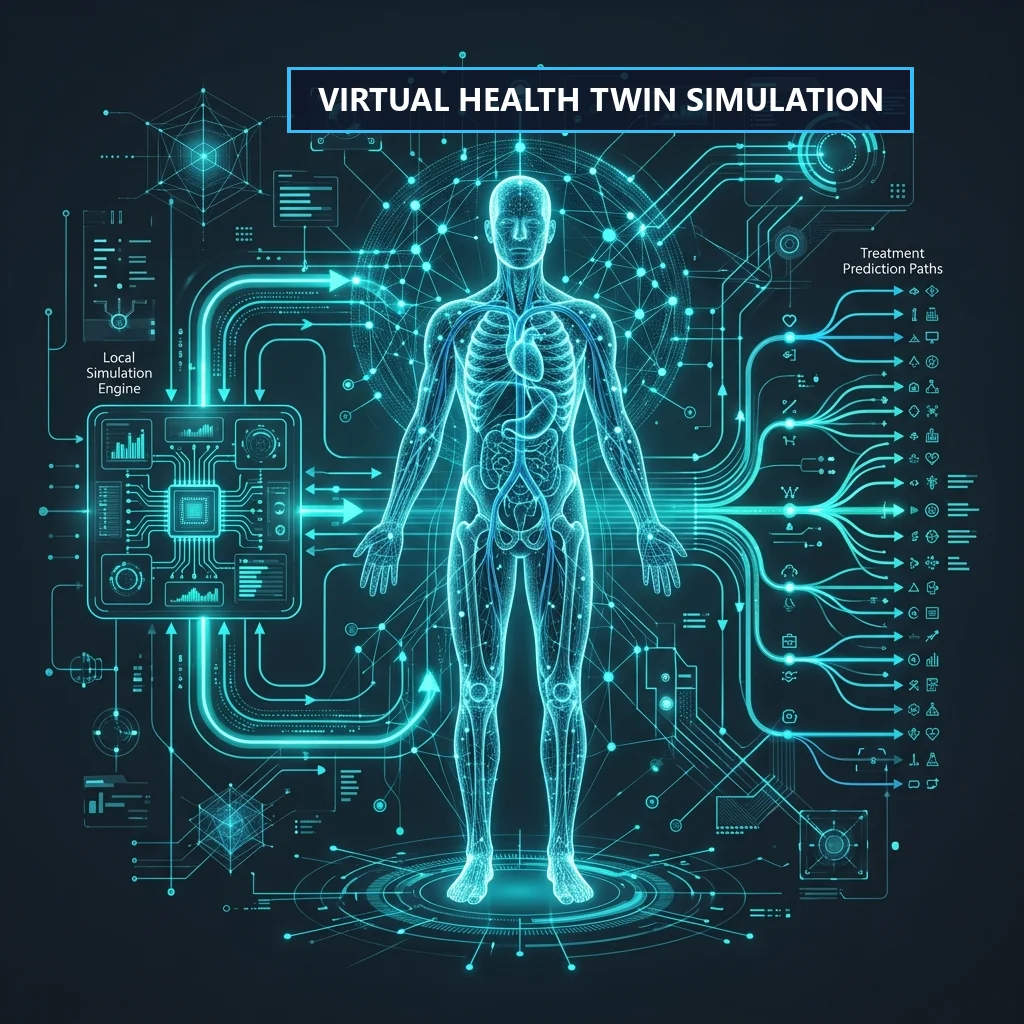
The Virtual Health Twin: Simulating Complex Treatments at the Edge
A virtual health twin is a real-time, dynamic digital model of a patient's biological systems, running locally at the compute edge. It goes beyond simple data logs by simulating how a patient's body will react to specific treatments before they are administered.
Local Simulation Loop
The virtual health twin requires tight integration between real-time vital feeds and predictive simulation engines.
+------------------+ +----------------------------+ +-------------------------+
| EHR & Vital | | Local Simulation Engine | | Treatment Prediction |
| Telemetry Logs | ======> | - Biological State Model | ======> | - Outcome Modeling |
| | | - Feedback Loops | | - Risk Classification |
+------------------+ +----------------------------+ +-------------------------+- State Ingestion: Real-time vital metrics (blood pressure, heart rate, blood gas levels) are streamed from local bedside monitors into the edge server.
- Biological Simulation: The simulation engine models the physiological response of the cardiovascular, respiratory, or nervous systems to potential drugs or procedures.
- Outcome Projection: The local model projects the risk of adverse reactions (such as acute kidney injury or arrhythmia) and highlights them to the clinical team.
Simulating Drug Interactions
Let us write a simulation script that models patient vitals under custom drug scenarios, running entirely on the localized node:
import numpy as np
class VirtualPatientTwin:
def __init__(self, baseline_bp: float, baseline_hr: float, systemic_resistance: float):
self.bp = baseline_bp # Mean arterial pressure (mmHg)
self.hr = baseline_hr # Heart rate (bpm)
self.resistance = systemic_resistance # Systemic vascular resistance index (SVRI)
self.state_history = []
def simulate_treatment(self, drug_name: str, dose_mg: float, steps: int = 10) -> list:
# Simulate local physiological reaction based on drug characteristics
states = []
current_bp = self.bp
current_hr = self.hr
current_res = self.resistance
for step in range(steps):
if drug_name == "Vasopressor":
# Increase vascular resistance, raising blood pressure
current_res += (dose_mg * 1.5) / (step + 1)
current_bp += (current_res * 0.1)
current_hr -= (step * 0.2) # Reflex bradycardia model
elif drug_name == "Beta-Blocker":
# Reduce heart rate and cardiac output
current_hr -= (dose_mg * 2.0) / (step + 1)
current_bp -= (dose_mg * 0.8) / (step + 1)
states.append({
"step": step,
"blood_pressure": round(current_bp, 2),
"heart_rate": round(current_hr, 2),
"vascular_resistance": round(current_res, 2)
})
return states
# Simulated execution at the ICU edge terminal
if __name__ == "__main__":
twin = VirtualPatientTwin(baseline_bp=65, baseline_hr=110, systemic_resistance=1200)
# Simulate vasopressor intervention to treat hypotension
projection = twin.simulate_treatment(drug_name="Vasopressor", dose_mg=5, steps=5)
print("Projected Physiological Response:")
for state in projection:
print(f"Step {state['step']}: BP={state['blood_pressure']} mmHg, HR={state['heart_rate']} bpm")Running these simulations locally allows clinicians to safely test complex drug protocols in real-time, with zero dependency on external network speeds.
Real-Time Pandemic Surveillance: Decentralized Global Safety Networks
Hospitals cannot operate as absolute silos. Tracking emerging infectious diseases, monitoring vaccine efficacy, and logging drug safety signals require global data sharing. How do we build global surveillance systems while protecting local patient privacy?
The answer lies in Decentralized Privacy-Preserving Networks.
Federated Learning and Encrypted Aggregation
Instead of pooling raw patient data into a central database, sovereign networks use federated architectures.
[ Local Hospital A ] ===> [ Local Model Fine-Tuning ] ===+
|
[ Local Hospital B ] ===> [ Local Model Fine-Tuning ] ===+===> [ Encrypted Aggregation Node ]
| (Anonymized Metadata Only)
[ Local Hospital C ] ===> [ Local Model Fine-Tuning ] ===+- Local Fine-Tuning: Each hospital runs local diagnostic models on its own patient data.
- Metadata Aggregation: The local models export anonymized weight updates and high-level trends (such as symptom search rate increases) to an external aggregation node.
- Global Model Sync: The aggregation node updates the global model weights and syncs them back to the edge systems, without ever seeing raw patient records.
To prevent indirect data leaks from model updates, we apply Differential Privacy by adding calibrated noise to the exported gradients, making it mathematically impossible to reconstruct the raw data of any single patient.
HIPAA/GDPR Access Control
To guarantee strict compliance, the data sharing pipeline is protected by access control layers. Every outbound update must pass through a local gateway that audits the data for any remaining identifiers.
Let us write a policy checking the data signature before allowing export to the network:
package healthcare.surveillance
# Deny update exports unless explicitly checked for anonymization and signed by local HSM
default allow_export = false
allow_export {
input.payload.is_anonymized == true
input.payload.data_integrity == "verified"
input.signature.valid == true
input.request.channel == "secure-federated-link"
contains_zero_phi_keys(input.payload.keys)
}
contains_zero_phi_keys(keys) {
# Prohibit raw patient identifiers from exiting local network
forbidden_keys := {"patient_name", "ssn", "medical_record_number", "dob", "address"}
intersection := keys & forbidden_keys
count(intersection) == 0
}This strict gateway guarantees that only verified metadata can leave the local environment.
Comparative Architecture: Legacy EMR vs. AI-Native Healthcare OS
To fully evaluate the shift to Predictive Sovereignty, we must compare the operational metrics of legacy Electronic Medical Records (EMRs) against an AI-Native Healthcare Operating System.
| Architectural Dimension | Legacy EMR Systems | AI-Native Healthcare OS (Edge) |
|---|---|---|
| Data Ingestion | Relational tables, batch HL7 sync (high latency) | Real-time FHIR streams, unstructured notes, vector databases |
| Privacy & Sovereignty | Centralized cloud DB or unencrypted local backups | Sovereign data lakes, micro-segmentation, local HSM controls |
| Latency & Reliability | High (500ms+ API roundtrip), dependent on WAN status | Microsecond (local memory bus), resilient to offline states |
| Compliance Model | Static periodic auditing, centralized database exposure | Real-time Cedar/OPA policies, Differential Privacy on exports |
| Clinical Decision Support | Static rule engines, warning boxes (high fatigue) | Real-time Virtual Health Twins, predictive diagnosis loops |
Futuristic Roadmap: The 2030 'Zero-Waiting-Room' Hospital
The ultimate goal of deploying an AI-Native Healthcare Cloud is the complete automation of the patient care pipeline, leading to the Zero-Waiting-Room Hospital. By shifting computing resources to the edge and embedding autonomous intelligence within secure boundaries, the patient journey is re-engineered from the ground up.
[ 2026 ] [ 2028 ] [ 2030 ]
+------------------+ +-------------------+ +---------------------+
| Legacy EMR Sync | ==> | Edge AI Agents | ======> | Fully Autonomous |
| & Vectorization | | & Local Pipelines | | Zero-Wait Hospital |
+------------------+ +-------------------+ +---------------------+- 2026: Local Foundation (Sovereignty Integration)
- Deconstruct relational database silos. Build local sovereign vector databases to aggregate clinical data.
- Run the first localized SLMs for real-time note summarization and data mapping.
- 2028: Agentic Coordination (Localized Autonomy)
- Deploy edge AI agents to coordinate clinical tasks: scheduling follow-ups, validating insurance pre-authorizations, and flagging drug interactions in real-time.
- Scale local virtual patient twins in ICU contexts to simulate pharmacological interventions.
- 2030: Zero-Waiting-Room Hospital (Full Execution)
- Fully integrate the clinical system. Patient arrival triggers local biometric validation and immediate check-in.
- Real-time diagnostic models analyze telemetry on-premises, instantly routing patients based on triage urgency.
- Administrative tasks (billing, coding mapping) are resolved on-premises immediately as care is delivered.
Actionable Close: Monday Morning Steps for MedTech Leaders
Transforming a legacy medical IT infrastructure into an AI-Native Healthcare Cloud is a multi-year journey, but the transition must begin immediately with concrete steps.
Step 1: Execute the Data Audit and Segment Metadata
Audit all clinical data streams. Identify key PHI fields and establish micro-segmented namespaces. Begin extracting unstructured medical logs into a local object store, laying the foundation for a sovereign patient data lake.
Step 2: Establish the Local Neural Compute Foundation
Set up high-density local edge compute nodes. Download and deploy quantized, domain-specific Small Language Models (SLMs) on local GPUs. Test key tasks (summarization, entity extraction) on-site to ensure zero reliance on external APIs.
Step 3: Implement Zero-Trust Policy Engines
Write and enforce programmatic access policies using OPA or Cedar. Place secure gateways around all local data boundaries, ensuring that all outgoing updates are fully anonymized before sharing.
block titled "Key Metric"
99.8% Latency Reduction: By moving clinical models from external cloud hosts to unified memory edge silicons, hospitals consistently drop inference roundtrip latencies from 500ms+ down to sub-10ms ranges, ensuring instant diagnostic responsiveness at the bedside.
