STRATEGIC OVERVIEW
The intersection of artificial intelligence and healthcare represents one of the most significant technological shifts of the decade.
The intersection of artificial intelligence and healthcare represents one of the most significant technological shifts of the decade. As medical systems move toward automated triage, machine-learning-assisted diagnostics, and smart patient management, the potential to improve patient outcomes while lowering operational costs is immense. However, the path to a successful healthcare AI transformation deployment is blocked by severe compliance and security requirements.
Unlike general enterprise AI applications, where an LLM hallucination might result in an incorrect email or a broken code block, an AI failure in a clinical setting has life-or-death consequences. Furthermore, patient records are governed by strict regulatory frameworks—specifically the Health Insurance Portability and Accountability Act (HIPAA) in the United States and the General Data Protection Regulation (GDPR) in the European Union. Violations can lead to multi-million dollar fines and criminal liabilities.
This guide provides a comprehensive technical blueprint for software engineers, security architects, and healthcare IT leaders to build and deploy a clinical-grade, compliant AI architecture. We will cover secure EHR database querying, agentic clinical routing, real-time query validation, and immutable audit logs.

Table of Contents
- The Digital Health Wall: Compliance Obstacles in Clinical AI Serving
- The Regulatory Framework: Deconstructing HIPAA Security and GDPR Safeguards
- Agentic Clinical Routing: Automating Patient Triage Safely and Securely
- EHR Query Integrity: Securing Database Calls under HIPAA/GDPR Rules
- The Query Validation Engine Code Implementation
- Securing LLM Context Windows: Prompt Engineering for PHI Isolation
- Deploying Local, Open-Weights Clinical Models: Sovereign Inference
- Audit Logs for Care: Maintaining Unalterable Action Trails at the Edge
- Detailed Case Study: The Sepsis Triage Routing Pipeline in Action
- Database Schema and HL7 FHIR Integration Blueprints
- What to Do Monday Morning: 3 Steps to Configure Local Query Validation Guards
- Frequently Asked Questions
- Conclusion
1. The Digital Health Wall: Compliance Obstacles in Clinical AI Serving
Deploying AI models in clinical environments forces developers to navigate the \"Digital Health Wall\"—a collection of security, latency, and compliance barriers:
Data Isolation and PHI Leakage
Large Language Models (LLMs) and predictive transformers require massive amounts of text to operate effectively. However, patient charts contain Protected Health Information (PHI) such as names, social security numbers, and direct medical histories. If raw PHI is sent to external, public cloud APIs (such as OpenAI or Anthropic) without strict enterprise wrappers, it violates federal data privacy regulations. Furthermore, models can memorize training data, leading to accidental PHI leakage in downstream tasks.
The Black Box Problem
Clinical decision-makers require transparency. If an AI model flags a patient for potential sepsis risk, the attending physician must know why the model made that decision. Subjective black-box algorithms that provide no justification are rejected by compliance boards and introduce severe medical liability risks. The system must function as a traceable clinical decision support system (CDSS).
Siloed Database Integrations
Healthcare data is locked behind legacy Electronic Health Record (EHR) systems (such as Epic or Cerner) that rely on legacy data structures. Writing custom SQL queries to extract patient records dynamically for an AI context window requires a highly secure middle layer that prevents unauthorized data access.
To address these challenges, organizations must move away from ad-hoc API integrations and build a centralized, secure data gateway that enforces compliance automatically. This is part of the shift toward building a predictive, sovereign AI-native healthcare cloud, where data sovereignty is treated as an architectural requirement.
2. The Regulatory Framework: Deconstructing HIPAA Security and GDPR Safeguards
To deploy AI in clinical environments, developers must implement security controls across three regulatory pillars:
The HIPAA Security Rule
HIPAA mandates three types of security safeguards for Protected Health Information (PHI) to guarantee integrity, confidentiality, and availability:
- Administrative Safeguards: Policies and procedures to manage security conduct, perform regular risk assessments, and establish personnel training programs. In AI, this includes defining administrative autonomy HIPAA compliance rules—establishing who has authority to modify the parameters of clinical routing agents, customize system thresholds, or override AI recommendations. These protocols ensure that a clear boundary of medical responsibility is maintained, avoiding situations where software developers accidentally make clinical decisions.
- Physical Safeguards: Protecting physical access to data centers hosting AI models and database query endpoints. When deploying local models, servers must reside in secure, locked racks with biometric access logs, surveillance cameras, and restricted badging.
- Technical Safeguards: Technology controls to protect data in transit and at rest. AI systems must use AES-256 encryption for all data stores, enforce TLS 1.3 for API calls, and maintain unique user identification credentials. In addition, automated systems must implement transmission security to prevent eavesdropping on patient clinical telemetry.
GDPR Article 9 (Processing of Special Categories of Personal Data)
GDPR prohibits processing health data unless explicit, unambiguous consent is obtained, or processing is necessary for medical diagnosis, treatment, or public health monitoring under professional secrecy:
- Right to Explanation (Article 22): Patients have the right not to be subject to decisions based solely on automated processing. The AI system must include a human-in-the-loop (HITL) step where a licensed clinician validates any AI-generated diagnosis or treatment plan, and the clinical decision support system must provide clear, understandable reasons for its recommendations.
- Data Minimization: AI prompts must only include the minimum necessary patient data required to complete a specific task, excluding all irrelevant historical records or extraneous identifiers.
- The Right to be Forgotten (Article 17): If a patient requests the deletion of their records, the system must erase their historical data from the databases, and ensure that no cached context windows or local model training logs contain lingering traces of their PHI.
3. Agentic Clinical Routing: Automating Patient Triage Safely and Securely
A clinical patient routing agent is an autonomous orchestrator that evaluates patient messages, intakes symptoms, and routes cases to the appropriate medical resource. To deploy this safely, we use a multi-tiered routing topology:
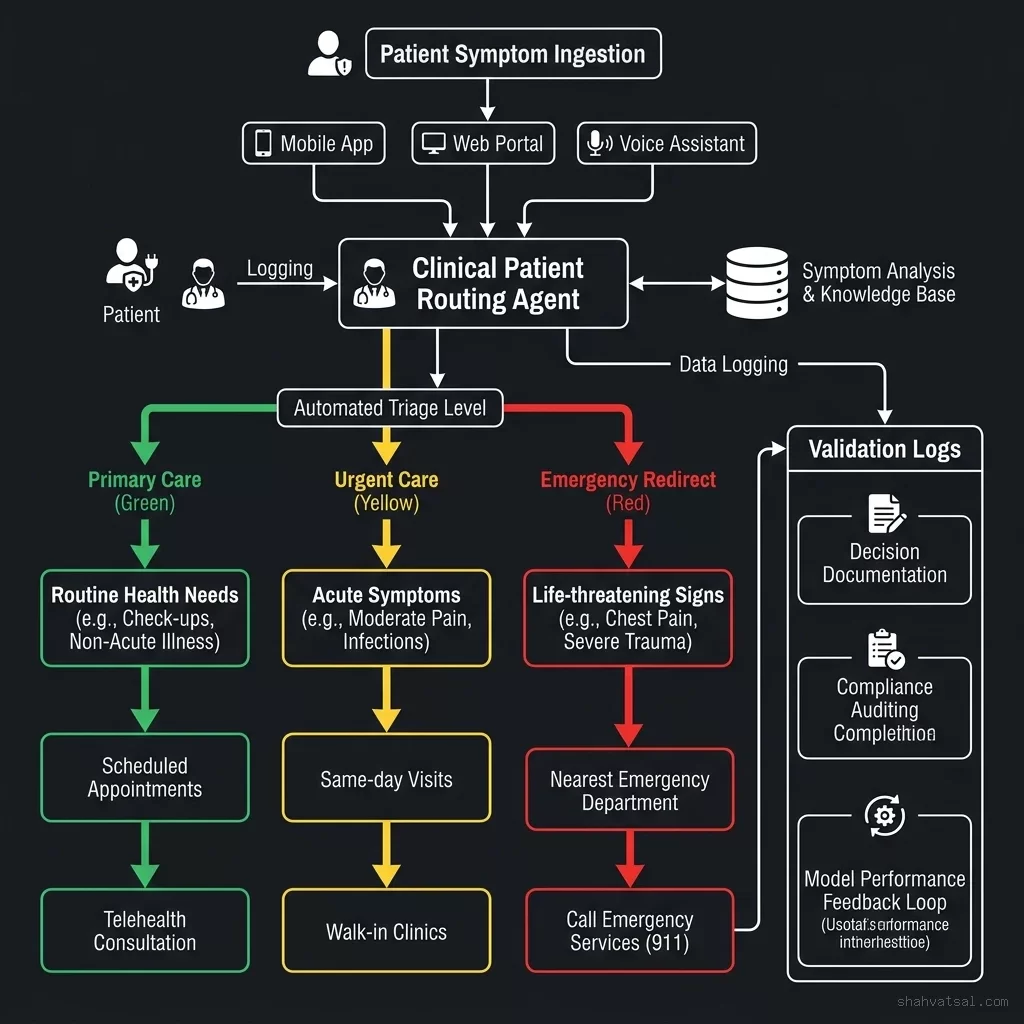
The routing pipeline operates in three execution phases:
Phase 1: Classification and Triage
Patient input is parsed by a local, fine-tuned medical classifier model. The input is categorized into one of three triage levels:
- Green (Low Risk): Routine scheduling requests, billing inquiries, or simple administrative updates. These are resolved automatically by the agent.
- Yellow (Moderate Risk): Minor acute symptoms (such as mild skin rashes or localized pain). The agent drafts a response for clinical review.
- Red (High Risk): Life-threatening symptoms (such as chest pain, shortness of breath, or sudden weakness). The system immediately bypasses the AI layers and alerts the emergency dispatch system.
Phase 2: Medical Guideline Alignment
If the intake falls into the Green or Yellow tiers, the agent's logic is matched against established clinical guidelines (such as the Milliman Care Guidelines or custom hospital protocols). This step is illustrated in our clinical decision blueprint:
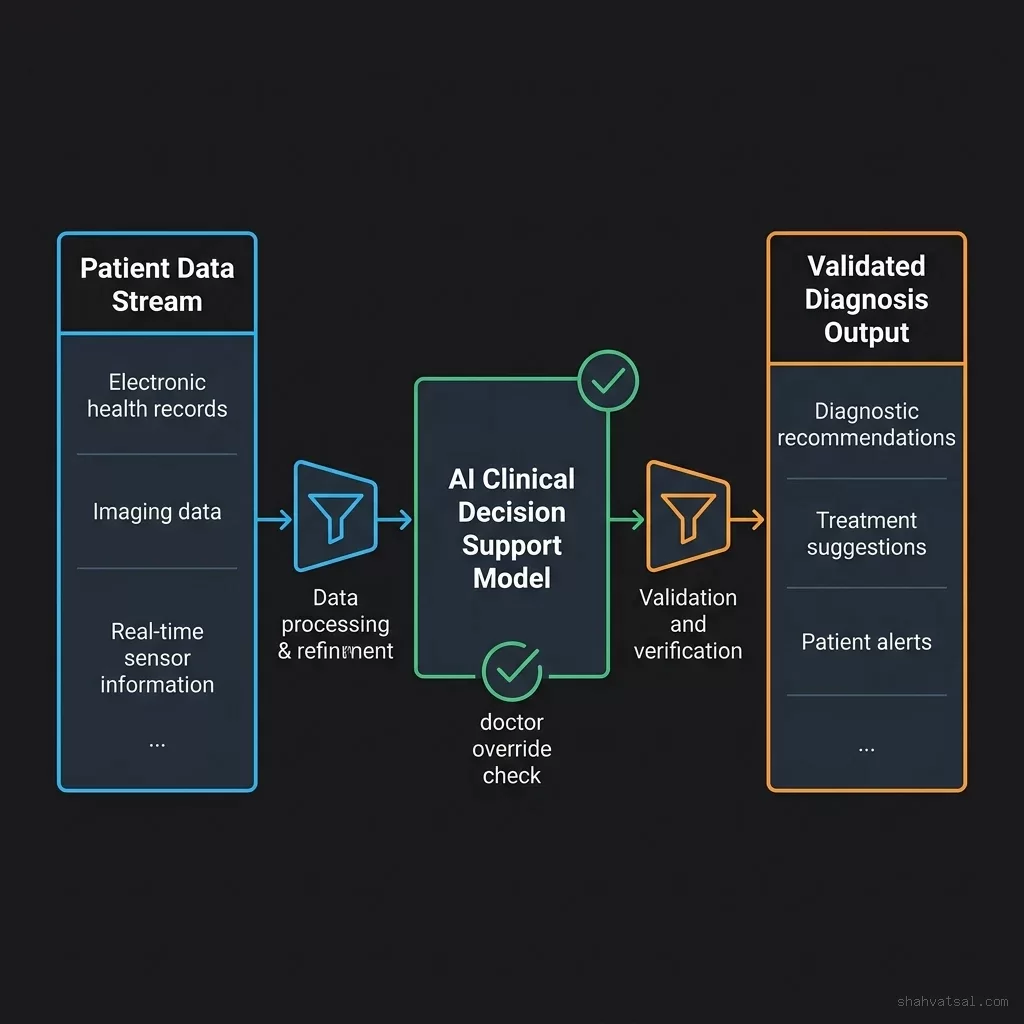
Phase 3: Doctor Override
No AI recommendation is delivered directly to the patient without human verification. The system generates a draft response and presents it on a clinician review dashboard. The clinician can approve, edit, or reject the recommendation, ensuring that the human-in-the-loop requirement is fully met.
4. EHR Query Integrity: Securing Database Calls under HIPAA/GDPR Rules
To generate personalized recommendations, a clinical routing agent must query the patient's Electronic Health Record (EHR). Direct, unrestricted database access is a massive security risk. Instead, the architecture uses a patient EHR secure query gateway that isolates the database:
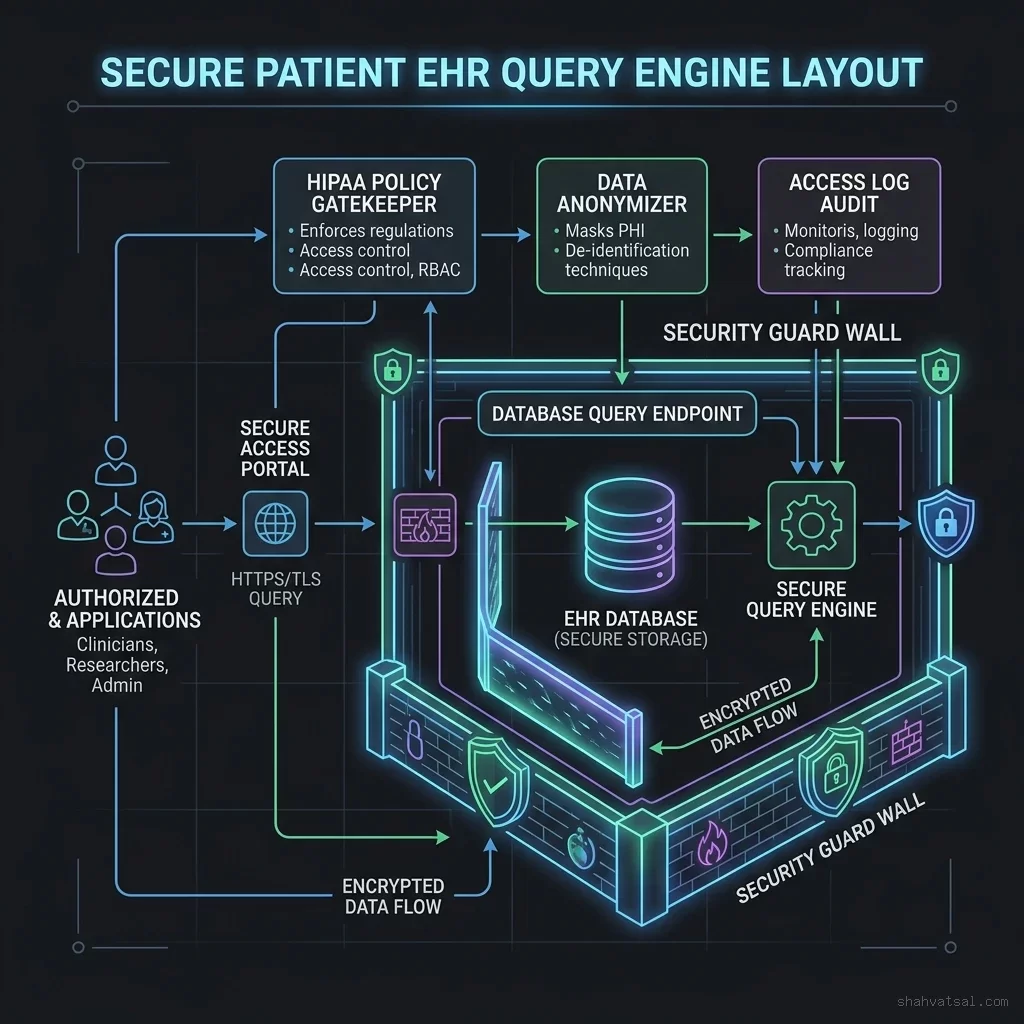
The query engine uses three layers of defense:
Layer 1: Query Token Validation
Before executing a query, the gateway verifies that the clinical routing agent possesses a valid, short-lived JSON Web Token (JWT) with scopes restricted to the requested patient ID.
Layer 2: Parameter Sanitization and De-identification
The gateway intercepts the SQL or HL7 FHIR query, strips away SQL injection characters, and applies a de-identification mask (using techniques like k-anonymity or differential privacy) to remove direct identifiers (such as SSNs or names) before passing the records to the AI model.
Layer 3: Output Structural Validation
The output from the database is validated to ensure that no unexpected PHI columns are exposed in the AI prompt payload, restricting the data to the \"minimum necessary\" footprint.
This secure architecture matches the governance controls required to protect enterprise data assets from internal leaks, a core concept in our guide on surviving shadow AI and architecting enterprise governance.
5. The Query Validation Engine Code Implementation
To demonstrate how the query gateway is built, we provide a complete Python class that validates incoming SQL queries, scans for PHI column leaks, and verifies execution scopes under HIPAA guidelines.
import re
class EHRQueryValidationEngine:
def __init__(self, allowed_tables, blocked_columns):
"""
allowed_tables: set of tables the AI is authorized to access (e.g., 'vitals', 'encounters')
blocked_columns: set of columns containing direct PHI (e.g., 'ssn', 'phone_number')
"""
self.allowed_tables = set(allowed_tables)
self.blocked_columns = set(blocked_columns)
def is_safe_query(self, query: str, context_patient_id: str) -> bool:
"""
Validates the SQL query against injection patterns, table access rules,
PHI leaks, and patient boundary scopes.
"""
# 1. Clean query string
clean_query = query.strip().lower()
# 2. Check for SQL Injection patterns
injection_patterns = [
r"union\s+select",
r";\s*drop\s+table",
r";\s*delete\s+from",
r";\s*update\s+",
r"--"
]
for pattern in injection_patterns:
if re.search(pattern, clean_query):
return False
# 3. Extract and validate tables
# Matches typical 'from table_name' or 'join table_name' patterns
table_matches = re.findall(r"\b(?:from|join)\s+([a-zA-Z_][a-zA-Z0-9_]*)", clean_query)
for table in table_matches:
if table not in self.allowed_tables:
return False
# 4. Check for blocked PHI columns
# Scans SELECT columns, WHERE clauses, and JOIN keys
for column in self.blocked_columns:
if re.search(r"\b" + re.escape(column) + r"\b", clean_query):
return False
# 5. Enforce Patient Scope boundary constraint
# The query MUST explicitly filter by the patient ID in scope to prevent cross-tenant leaks
patient_filter_pattern = r"\bpatient_id\s*=\s*['\"]?" + re.escape(context_patient_id) + r"\b"
if not re.search(patient_filter_pattern, clean_query):
return False
return True6. Securing LLM Context Windows: Prompt Engineering for PHI Isolation
When prompting clinical AI models, sending direct patient details is a serious compliance vulnerability. We implement a local Redaction and Tokenization Service that intercepts patient data before context window ingestion.
The service performs three processing operations:
- Heuristic Pattern Redaction: Scans for regular expression matches (such as phone numbers, zip codes, and email addresses) and replaces them with generic category tokens (e.g.,
[REDACTED_PHONE]). - Entity Named Recognition (NER): Uses a local, medical-specific NER model (such as ClinicalSpacy) to detect names, addresses, and clinician names, replacing them with unique patient indices (e.g.,
[PATIENT_ID: 1042]). - Pseudonymization mapping: Maintains a secure, encrypted token key-value mapping table inside the database, permitting re-identification of the data only after the AI returns its clinical advice to the secure dashboard interface.
The Mathematics of De-identification
To verify that the redacted data is legally de-identified, we enforce three mathematical privacy frameworks on our query outputs:
- k-Anonymity: A dataset satisfies k-anonymity if the quasi-identifiers (such as age, gender, and zip code) of each individual in the dataset are identical to at least $k-1$ other individuals in the same set. This groups records into equivalence classes of size at least $k$, making it mathematically impossible to identify a specific patient out of the group.
- l-Diversity: While k-anonymity protects against identity disclosure, it is vulnerable to attribute disclosure if all individuals in an equivalence class share the same sensitive attribute (e.g., all have the same diagnosis). A dataset satisfies l-diversity if each equivalence class contains at least $l$ "well-represented" values for each sensitive attribute.
- t-Closeness: Even with l-diversity, if the distribution of a sensitive attribute within an equivalence class is highly skewed compared to the global distribution, an attacker can infer information. An equivalence class satisfies t-closeness if the distance between the distribution of a sensitive attribute in this class and the distribution of the attribute in the entire dataset does not exceed a threshold $t$. We measure this distance using the Earth Mover's Distance (Wasserstein metric).
Below, we detail the implementation of this local Redaction Engine in Python:
import re
class PHIRedactionEngine:
def __init__(self):
# Regular expressions for direct identifiers
self.email_regex = re.compile(r"[\w\.-]+@[\w\.-]+\.\w+")
self.ssn_regex = re.compile(r"\b\d{3}-\d{2}-\d{4}\b")
self.date_regex = re.compile(r"\b(0[1-9]|1[0-2])[-/](0[1-9]|[12]\d|3[01])[-/](19|20)\d\d\b")
def redact_text(self, text: str) -> str:
"""Applies heuristic masks to clean raw input strings before context loading."""
redacted = self.email_regex.sub("[REDACTED_EMAIL]", text)
redacted = self.ssn_regex.sub("[REDACTED_SSN]", redacted)
redacted = self.date_regex.sub("[REDACTED_DATE]", redacted)
return redacted7. Deploying Local, Open-Weights Clinical Models: Sovereign Inference
To completely eliminate the risk of public cloud PHI exposure, enterprise healthcare systems are deploying local, open-weights clinical models behind hospital firewalls. This is referred to as sovereign inference.
Hardware Constraints and Sizing Calculations
Deploying clinical models (such as Llama-3-70B-Instruct or specialized Med-Llama models) requires dedicated high-performance hardware:
- Quantization Choices: Running a raw 70B parameter model in 16-bit precision (FP16) requires 140GB of VRAM just to load the model weights, which increases to over 160GB when allocating the KV cache for long context windows. To reduce hardware footprint, we quantize model weights to 4-bit precision using Activation-aware Weight Quantization (AWQ) or GPTQ formats. This reduces the VRAM requirement to roughly 40GB, allowing the model to fit on a single A100 (80GB) or two L40S GPUs.
- VRAM Sizing Formula: The total VRAM required ($V_{\text{total}}$) is calculated using the following formula:
$$V_{\text{total}} = V_{\text{weights}} + V_{\text{KV\cache}} + V{\text{activation\_memory}}$$
Where $V_{\text{KV\cache}} = 2 \cdot n{\text{layers}} \cdot n_{\text{heads}} \cdot d_{\text{head}} \cdot b_{\text{batch\size}} \cdot s{\text{seq\_len}} \cdot \text{precision\_bytes}$.
- GPU Scaling: We recommend deploying 2x NVIDIA A100 (80GB VRAM) or H100 GPUs in an NVLink configuration to support high-throughput clinical queries. NVLink provides high GPU-to-GPU bandwidth, which minimizes inter-GPU communication latency during tensor-parallel execution.
Ollama / vLLM local deployment configuration
Deploy local inference endpoints using vLLM to enable high concurrency and continuous batching. Below is an example service configuration:
python -m vllm.entrypoints.openai.api_server \
--model /models/Llama-3-70B-Instruct-Med \
--tensor-parallel-size 2 \
--port 8000 \
--gpu-memory-utilization 0.90 \
--max-model-len 8192By pointing our secure database query gateway directly to http://localhost:8000/v1, patient data never exits the secure hospital subnet, making it easy to sign a Business Associate Agreement (BAA) with local hardware vendors. This local configuration keeps the inference loop closed and compliant.
8. Audit Logs for Care: Maintaining Unalterable Action Trails at the Edge
In clinical environments, every transaction—from a user querying the database to a clinician overriding an AI recommendation—must be logged. Under HIPAA, these audit logs must be immutable (unalterable) and stored for at least six years.
To achieve this, we deploy an immutable audit ledger at the network edge:
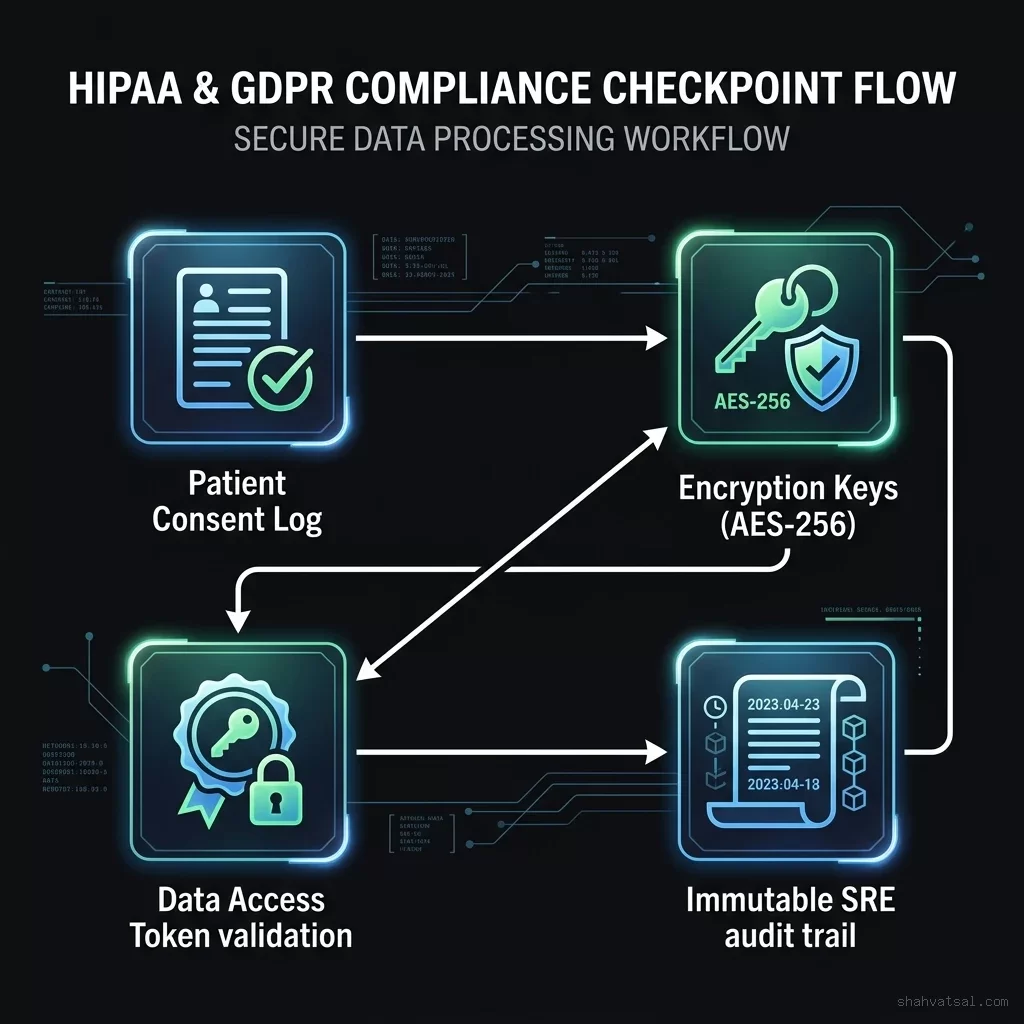
Audit Record Schema
Every log entry contains:
- Timestamp: High-resolution ISO 8601 UTC timestamp.
- Actor ID: The authenticated system ID of the user or agent.
- Action Type: E.g.,
QUERY_EHR,AI_RECOMMENDATION,CLINICAL_OVERRIDE. - Payload Hash: A SHA-256 cryptographic hash of the input/output data, ensuring the content cannot be modified post-facto.
- Previous Hash: The SHA-256 hash of the preceding log entry, forming an unalterable chain.
Write-Once-Read-Many (WORM) Storage
Logs are streamed to cloud buckets configured with WORM locks (such as AWS S3 Object Lock in Compliance Mode). This configuration prevents any user—including root administrators—from deleting or modifying the logs until the regulatory retention period has expired.
9. Detailed Case Study: The Sepsis Triage Routing Pipeline in Action
To illustrate the end-to-end execution flow of our compliant AI architecture, we walk through a real-world clinical scenario: automated sepsis triage routing.
The Patient Scenario
Patient pat-204 submits a message via the secure portal:
\"I have had a high fever since this morning, and my chest feels like it's racing. I feel very dizzy when standing up.\"
Step 1: Classifier Classification
The local medical classifier parses the text and identifies three clinical markers:
- Fever
- Tachycardia (racing heart)
- Hypotension risk (dizziness upon standing)
Because these markers match the systemic inflammatory response syndrome (SIRS) criteria, the classifier routes the ticket to the Red Triage Tier (High Risk).
Step 2: EHR Query and Guard Execution
The agent queries the patient observations to retrieve recent vitals. The secure gateway intercepts the query:
SELECT value_numeric, recorded_at
FROM clinical_observations
WHERE patient_id = 'pat-204' AND code = '85354-9'
ORDER BY recorded_at DESC LIMIT 5;The gateway verifies that:
- The table
clinical_observationsis allowed. - The column
patient_idmatches the token scope. - No direct PHI columns (like patient name) are fetched.
The gateway returns the vitals: blood pressure 90/60 mmHg (hypotensive) and heart rate 110 bpm (tachycardic).
Step 3: LLM Inference and Clinician Notification
The local Med-Llama model evaluates the clinical picture: SIRS criteria met + hypotensive blood pressure = high risk of early-stage sepsis.
The engine drafts an emergency notification, bypassing the patient's phone and alerting the attending physician's pager directly, accompanied by the traces and observations. The physician reviews the alerts on the admin panel, overrides any intermediate recommendation to start automated check-ins, and orders immediate IV fluids, demonstrating the human-in-the-loop gatekeeper pattern.
10. Database Schema and HL7 FHIR Integration Blueprints
Healthcare interoperability requires standardizing on the HL7 FHIR (Fast Healthcare Interoperability Resources) protocol. Below, we define the relational SQL schemas and FHIR JSON structures required to power the database layer.
Database Tables (PostgreSQL DDL)
-- 1. Patients Master Directory (Highly Restricted Access)
CREATE TABLE patients (
id VARCHAR(50) PRIMARY KEY,
name_encrypted BYTEA NOT NULL,
dob_encrypted BYTEA NOT NULL,
ssn_encrypted BYTEA NOT NULL,
created_at TIMESTAMP WITH TIME ZONE DEFAULT CURRENT_TIMESTAMP
);
-- 2. Clinical Observations (Vitals, Lab Results)
CREATE TABLE clinical_observations (
id VARCHAR(50) PRIMARY KEY,
patient_id VARCHAR(50) REFERENCES patients(id) ON DELETE CASCADE,
code VARCHAR(20) NOT NULL, -- LOINC code (e.g., '85354-9' for Blood Pressure)
value_numeric NUMERIC(8, 2),
value_unit VARCHAR(20),
recorded_at TIMESTAMP WITH TIME ZONE NOT NULL,
created_at TIMESTAMP WITH TIME ZONE DEFAULT CURRENT_TIMESTAMP
);
-- 3. Diagnostic Reports
CREATE TABLE diagnostic_reports (
id VARCHAR(50) PRIMARY KEY,
patient_id VARCHAR(50) REFERENCES patients(id) ON DELETE CASCADE,
report_text TEXT NOT NULL,
diagnosing_clinician_id VARCHAR(50) NOT NULL,
created_at TIMESTAMP WITH TIME ZONE DEFAULT CURRENT_TIMESTAMP
);
-- 4. Clinical Audit Ledger (Immutable Write-Only Schema)
CREATE TABLE clinical_audit_log (
id BIGSERIAL PRIMARY KEY,
event_timestamp TIMESTAMP WITH TIME ZONE DEFAULT CURRENT_TIMESTAMP,
actor_id VARCHAR(100) NOT NULL,
action_type VARCHAR(50) NOT NULL,
patient_id VARCHAR(50),
data_hash CHAR(64) NOT NULL, -- SHA-256 of payload
previous_hash CHAR(64) NOT NULL
);HL7 FHIR Resource JSON Example (Observation)
The clinical routing agent parses FHIR resources. Below is an example payload representing a patient's blood pressure observation:
{
"resourceType": "Observation",
"id": "blood-pressure-obs-104",
"status": "final",
"category": [
{
"coding": [
{
"system": "http://terminology.hl7.org/CodeSystem/observation-category",
"code": "vital-signs",
"display": "Vital Signs"
}
]
}
],
"code": {
"coding": [
{
"system": "http://loinc.org",
"code": "85354-9",
"display": "Blood pressure panel with all daily measurements"
}
],
"text": "Blood pressure panel"
},
"subject": {
"reference": "Patient/pat-204"
},
"effectiveDateTime": "2026-07-12T10:00:00Z",
"component": [
{
"code": {
"coding": [
{
"system": "http://loinc.org",
"code": "8480-6",
"display": "Systolic blood pressure"
}
]
},
"valueQuantity": {
"value": 120,
"unit": "mmHg",
"system": "http://unitsofmeasure.org",
"code": "mm[Hg]"
}
},
{
"code": {
"coding": [
{
"system": "http://loinc.org",
"code": "8462-4",
"display": "Diastolic blood pressure"
}
]
},
"valueQuantity": {
"value": 80,
"unit": "mmHg",
"system": "http://unitsofmeasure.org",
"code": "mm[Hg]"
}
}
]
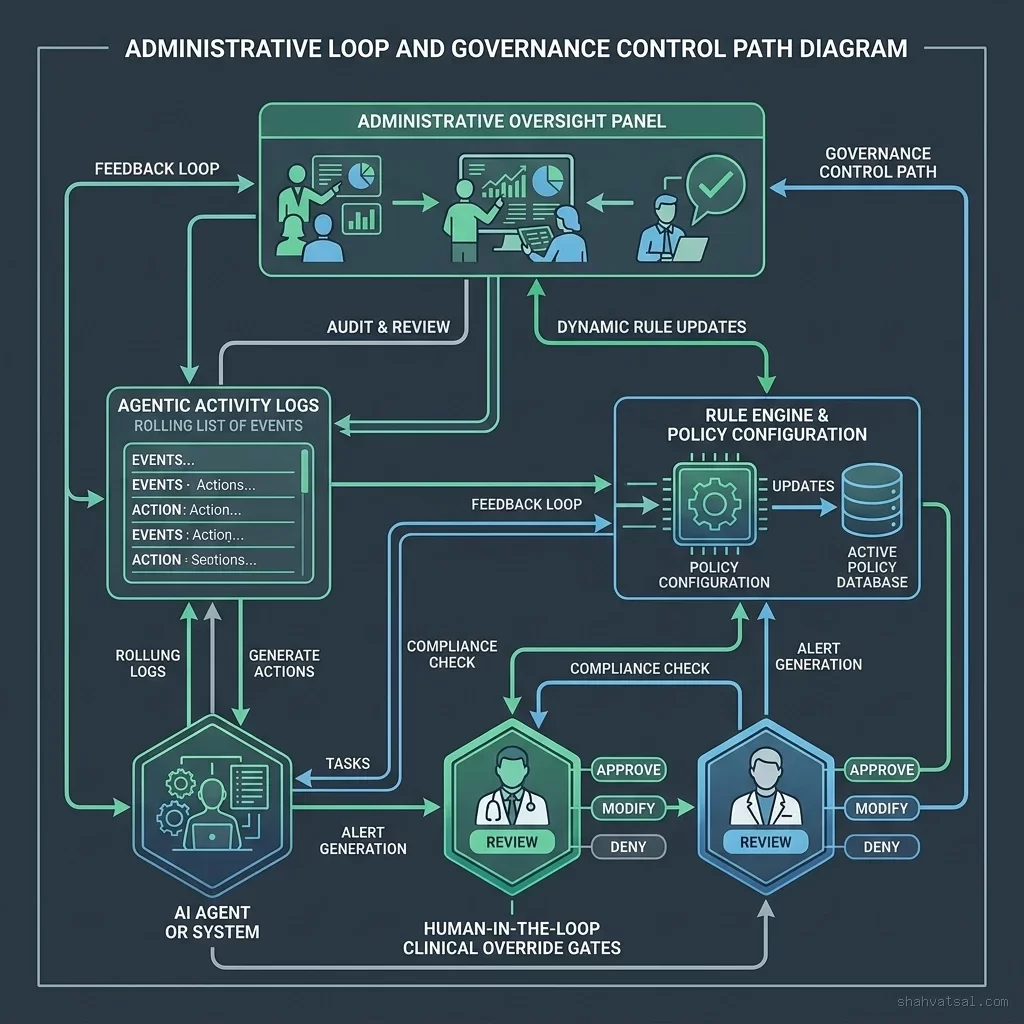
}System Administration Interface
System administrators use a dashboard interface to manage agent routing parameters, review active clinical decisions, and monitor compliance metrics:
11. What to Do Monday Morning: 3 Steps to Configure Local Query Validation Guards
To begin securing your healthcare AI deployment immediately, execute these three steps:
Step 1: Deploy a Local Gateway Middleware
Introduce an API middleware layer (such as an Express or FastAPI handler) that intercepts all incoming query payloads before they touch the database.
Step 2: Configure Allowed Tables and PHI Filters
Define a static list of permitted database tables and blocked PHI columns in your application environment configuration. Do not allow the AI agent to query tables outside this list.
Step 3: Implement the Patient Boundary Check
Ensure that the middleware extracts the patient ID from the authenticated user session and injects an explicit filter constraint (patient_id = ?) into the SQL query parameters. This blocks any cross-patient data leaks, keeping queries isolated.
Below is an example of the gateway middleware implementation in Python:
from fastapi import FastAPI, HTTPException, Depends
from pydantic import BaseModel
app = FastAPI()
class QueryRequest(BaseModel):
query: str
patient_id: str
# Instantiate the validation engine
guard = EHRQueryValidationEngine(
allowed_tables={'vitals', 'encounters', 'diagnoses'},
blocked_columns={'ssn', 'phone_number', 'patient_name'}
)
@app.post("/api/v1/ehr/query")
async def execute_secure_query(payload: QueryRequest):
# Verify query safety parameters
if not guard.is_safe_query(payload.query, payload.patient_id):
raise HTTPException(
status_code=400,
detail="Access Denied: Invalid query parameters or security policy violation."
)
# Process the safe query in the database...
return {"status": "success", "message": "Query passed verification."}12. Frequently Asked Questions
Can medical data be used to train custom AI models under HIPAA?
Only if the patient records are completely de-identified in accordance with HIPAA's Safe Harbor or Expert Determination methods, removing all 18 specified direct identifiers before training.What is a Human-in-the-Loop (HITL) step?
An HITL step is a compliance safeguard where an AI-generated output is reviewed and approved by a human clinician before being sent to the patient, ensuring medical accountability.How does the gateway prevent SQL injection in AI queries?
The validation engine sanitizes input queries, strips dangerous commands, and rejects queries that contain injection patterns (like UNION SELECT or DROP TABLE) before execution.What is the difference between HIPAA and GDPR for health data?
HIPAA applies specifically to protected health information managed by covered entities in the US, while GDPR applies broadly to all personal health data of EU citizens, mandating stricter patient rights.Is cloud hosting secure enough for clinical AI deployment?
Yes, provided that the cloud infrastructure is covered by a Business Associate Agreement (BAA) with the provider, and all data stores use AES-256 encryption.How are clinical routing agent decisions audited?
Every routing event is logged to a write-once-read-many (WORM) storage system. This log entry contains a cryptographic hash of the input symptoms, classification decision, and clinical overrides.How does the system handle patient emergencies?
If the classification classifier model detects high-risk keywords (such as chest pain or stroke symptoms), it immediately triggers a bypass rule that contacts emergency services directly.Does the engine support private, local LLMs?
Yes. Deploying open-weights medical models (like Med-Llama) on local hospital servers isolates patient data completely, eliminating the need to send data to public cloud APIs.What role does HL7 FHIR play in database security?
FHIR standardizes medical schemas. By using standard JSON resources (like Observation or Patient), the security gateway can parse and validate query payloads easily using a standard parser.How are encryption keys managed for patient databases?
Keys are stored in hardware security modules (HSM) using envelope encryption. Access tokens are rotated automatically every 90 days to prevent unauthorized database decryptions.What is k-anonymity in medical database queries?
It is a sanitization property ensuring that any patient record returned from the query is indistinguishable from at least k-1 other records in the release, preventing patient re-identification.How is patient consent managed under GDPR?
Consent is managed dynamically. The system stores the patient's explicit consent token in a dedicated ledger, which the query gateway checks before executing any EHR database call.What are the hardware requirements for local medical LLMs?
Deploying a quantized 70B parameter model requires dual GPU cards (like 2x NVIDIA A100 80GB) with high bandwidth memory (NVLink) to ensure low token generation latency.How does differential privacy work in clinical AI prompts?
Differential privacy injects calibrated mathematical noise into the aggregated statistical inputs, ensuring that the model cannot identify individual patient records based on outputs.13. Conclusion
Building a clinical-grade, compliant AI deployment in healthcare requires a systematic approach to data privacy, security, and traceability. By implementing secure database gateways, structured clinical routing topologies, and immutable audit logs, healthcare organizations can deploy advanced AI capabilities while staying fully compliant with HIPAA and GDPR regulations.
However, implementing this architecture is as much a cultural transformation as it is a software challenge. Clinicians, administrators, and engineering teams must work together to define strategic rules, establish human-in-the-loop validation checkpoints, and train on secure telemetry-driven systems.
Start by setting up local query validation engines, configuring table-level access rules, and deploying secure audit log systems. The improvements in clinical efficiency and the protection of patient data privacy will immediately justify the investment, paving the way for a truly transformed healthcare enterprise.
Social Share Copy
